We all experience hair loss, losing between 50 and 100 strands of hair daily. Hair is lost as a result of a new hair growing in the follicle and pushing the older hair out. Hair grows in a pattern that consists of 3 stages: growth (anagen), involution (catagen), and rest (telogen). At any one time, 90-95% of hairs are in the anagen phase, 1% are in catagen and 5-10% of hairs in telogen. Most hair shedding tends to occur in the telogen phase.
A little hair loss is normal. Excessive hair loss although not typical, is extremely common. Excessive hair loss diseases may include the entirety of the scalp (diffuse alopecia), it may occur in patches (patchy alopecia), or it may be limited to specific regions (patterned alopecia, marginal alopecia).
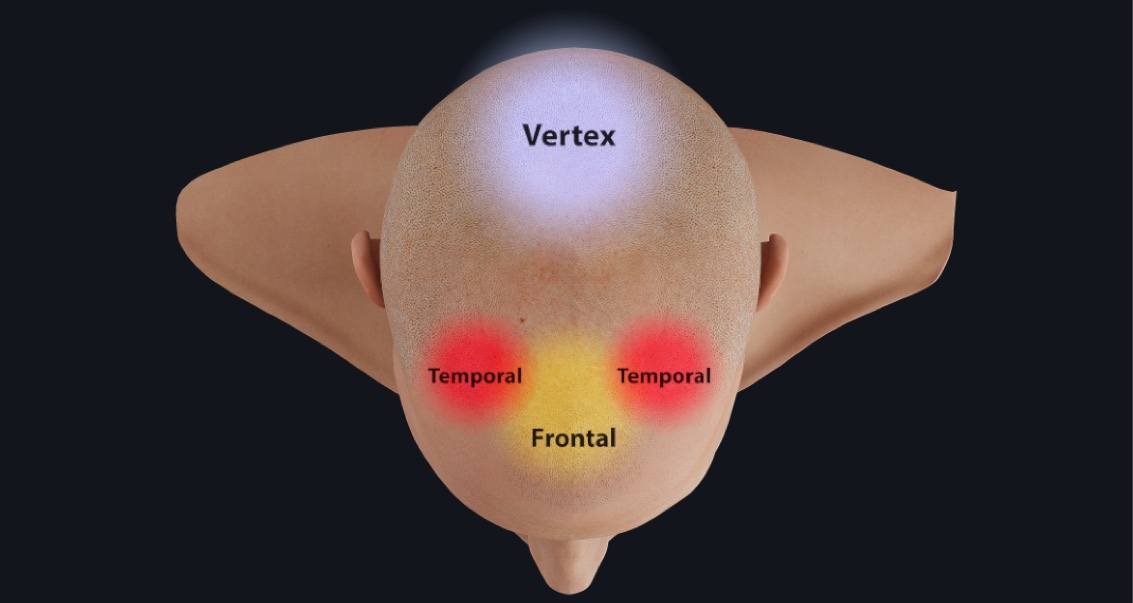
The most common type of hair loss is androgenetic/androgenic alopecia or pattern baldness. It affects up to 80% of men and 50% of women. It is a genetically predetermined disease that tends to worsen with time, affecting the diameter, length, and pigmentation of hair. Unlike other alopecia- related diseases, androgenic alopecia is limited to the frontal, temporal and vertex areas.
The cause of androgenic alopecia is thought to result from hair follicles developing an abnormal response to dihydrotestosterone (DHT). DHT is an androgen and sex steroid. Like other androgens, it regulates and maintains male characteristics. In this case, the hormone causes miniaturization of hairs, resulting in thinner, smaller hairs. There is no loss of hair follicles or scarring, but hair does appear considerably thinner. As we already mentioned, this type of hair loss is focused in specific areas, in particular the frontal, temporal, and vertex areas. This is because the hair follicles in these areas are particularly sensitive to the effects of DHT.
The exact mechanism behind this process is unclear however DHT is now a common therapeutic target to effectively treat baldness. Finasteride is the primary DHT blocker, it inhibits the production of DHT, halting hair loss and encouraging regrowth.